Imaging case 14:
Breast Cancer - Ductal Carcinoma In Situ
During breast-conserving surgery it is common practice to perform intraoperative assessment of the resected tumor specimen to assess if the resection was successful. This is especially useful for patients diagnosed with Ductal Carcinoma In Situ (DCIS), as the positive margin rate is higher in this population. The most frequently used techniques such as specimen radiography or frozen section assessment all have their drawbacks regarding performance and/or efficiency.
In this clinical case, which is part of the multi-center prospective BrIMA study (NCT04999917), we highlight how intraoperative specimen PET-CT imaging can bring more confidence into the operating room. This gives the surgeon a clear view of what was resected – and the ability to act upon this information at the point of surgery.
Patient History
A 66-year old woman with Ductal Carcinoma In-Situ(DCIS) underwent breast-conserving surgery. The tumor size on preoperative imaging was 30mm, biopsy showed a grade 3 tumor, receptor status unknown. Preoperative staging was cTisN0M0.
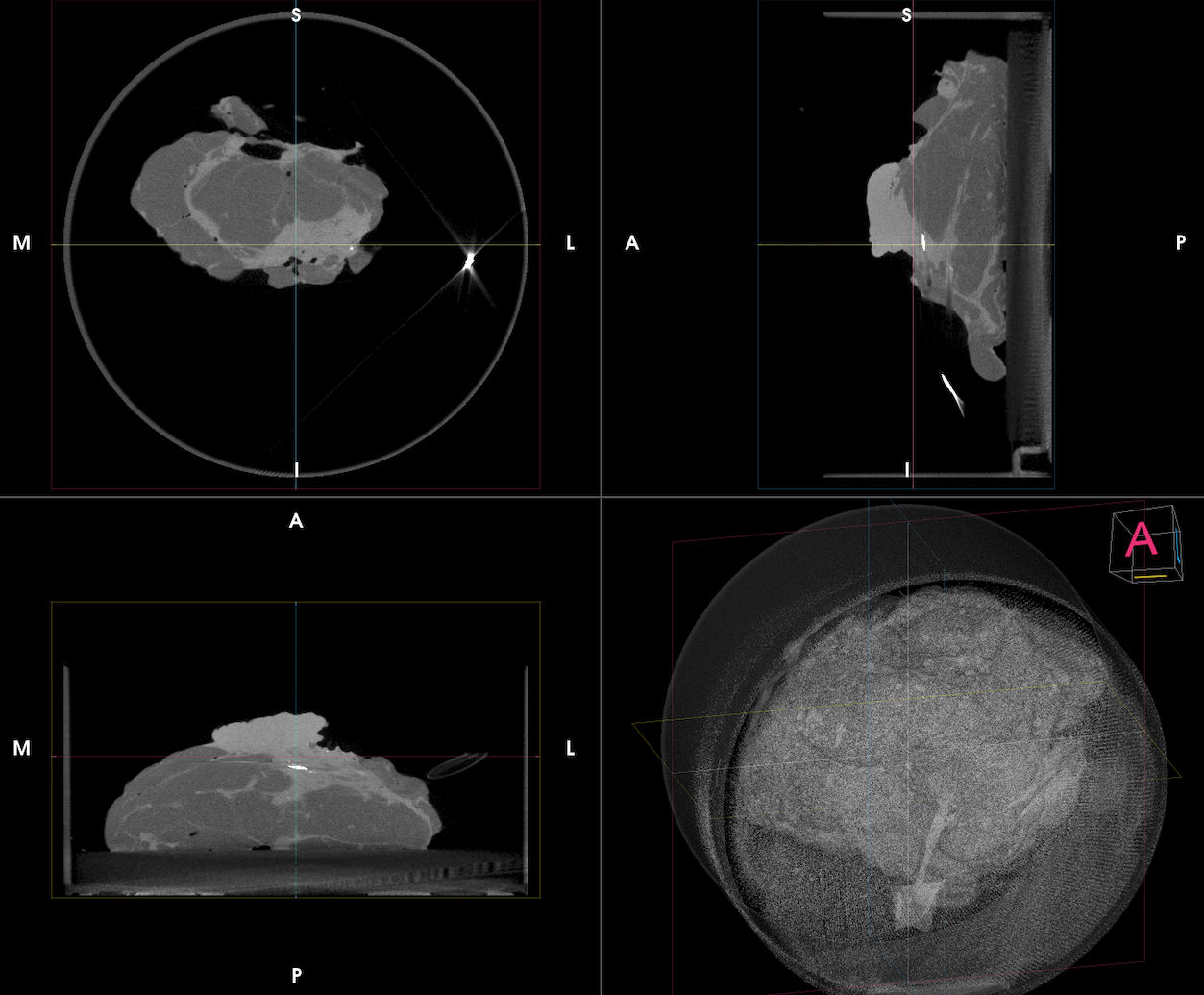 Figure 1. Coronal, sagittal and transverse slices of the CT images of a DCIS. A dense lump is visualized in the inferior region of the specimen.
Figure 1. Coronal, sagittal and transverse slices of the CT images of a DCIS. A dense lump is visualized in the inferior region of the specimen.
PET-CT specimen images
An intravenous injection with 70 MBq (0.80 MBq/Kg) of 18F-FDG was given on the morning of the surgery at the Nuclear Medicine Department. The patient was then transferred to the operating theatre and breast-conserving surgery was performed per standard protocol.
The resected breast specimen was imaged immediately after resection and the images were interpreted by the surgeon in the operating room. This was approximately 103 min after 18F-FDG injection.
Per-op specimen mammography (RX) showed that all margins were negative, so no oriented cavity shaving was recommended. The CT (Fig. 1) visualizes the entire specimen in 3D and more dense tissue was visible in the inferior region of the specimen. his already provides an indication of where the tumor is located in the specimen. Microcalcifications can be observed due to the high spatial resolution (100µm) of the CT image.
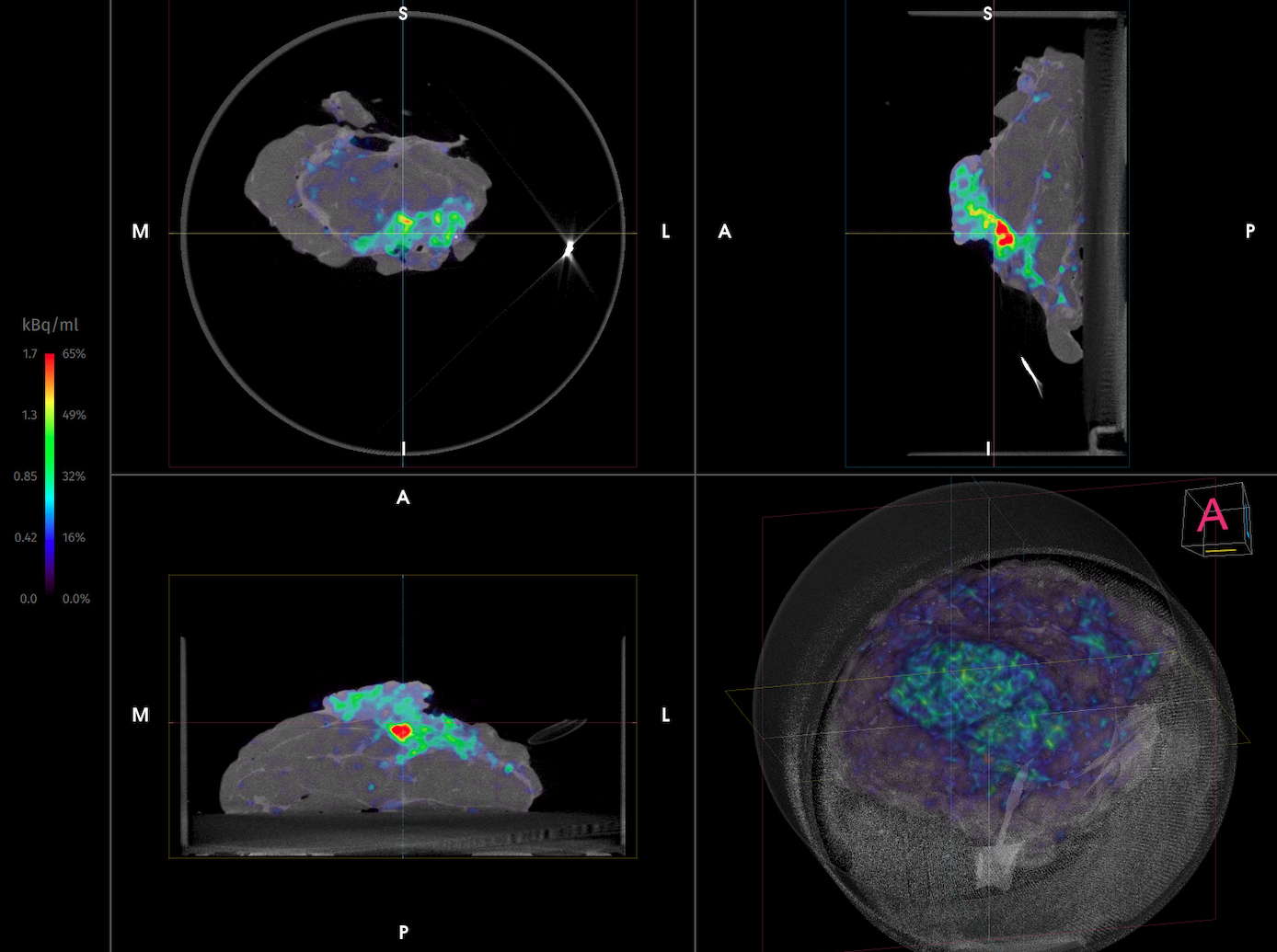
Figure 2. Coronal, sagittal and transverse slices of the PET-CT images of a DCIS. Showing increased 18F-FDG uptake at the inferior border. Postoperative final pathology showed that there was only a tumor-free margin of <1mm at the inferior side. Specimen orientation is as indicated.
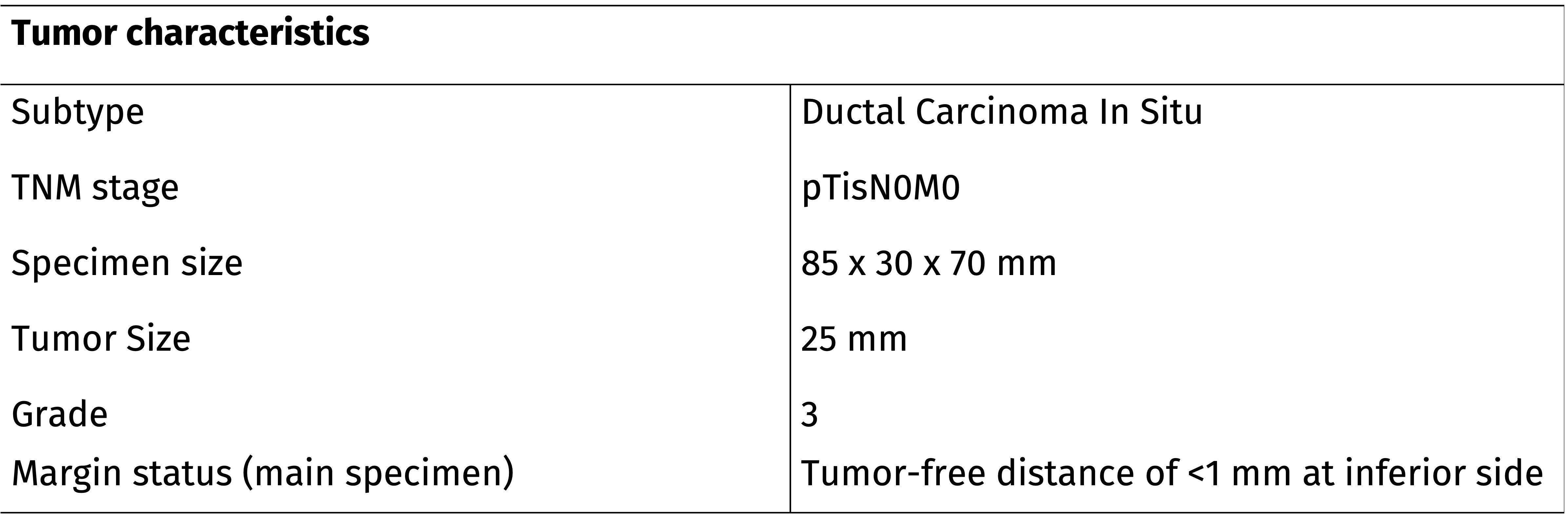 Table 1. A summary of the histopathological findings of the resected specimens.
Table 1. A summary of the histopathological findings of the resected specimens.
Histopathological Evaluation
Immediately after specimen imaging, the resected specimen was sent to the pathology department for routine histopathological evaluation, which was available after several days. Table 1 shows the results of histopathology. Postoperative final pathology showed that there was only a tumor-free margin of <1mm at the inferior side, where 2mm tumor-free margin is required in BCS for DCIS.
Discussion and Conclusion
In this interesting case, the surgeon decided to perform an additional cavity shave based on specimen PET-CT imaging as 18F-FDG uptake was reaching the inferior border of the specimen. Histopathological evaluation also showed only a tumor-free margin of <1 mm was reached at the inferior border. In this patient the additional cavity shave helped to avoid the need for reoperation and the associated burden.
REFERENCES
St John et al, Diagnostic Accuracy of Intraoperative Techniques for Margin Assessment in Breast Cancer Surgery: A Meta-analysis. Ann Surg 2017.