Imaging Case 19:
Prostate cancer - Adenocarcinoma
Radical prostatectomy often requires sacrificing the neurovascular bundle, which can significantly impact a patient's quality of life, particularly in terms of sexual function and loss of continence. A nerve-sparing approach aims to preserve these structures and reduce the risk of postoperative impotence and incontinence, but it comes with an increased risk of incomplete tumor removal. Therefore, having real-time insights on whether the tumor has been fully resected is highly valuable during nerve-sparing surgery. Recent publications have shown that high-resolution specimen PET-CT imaging may provide such insights [1,3,4,5].
In this case, we illustrate how intraoperative specimen PET-CT imaging with 18F-PSMA allows visualizing the tumor in the resected tissue specimen. This real-time assessment could assist the surgeon in determining whether additional tissue removal is necessary, ultimately improving surgical precision and patient outcomes.
This case is presented with the support of dr. B. Lambert, Prof. dr. K. Decaestecker, dr. F. Ameye, dr. P. De Backer, and colleagues of AZ Maria Middelares hospital, Ghent, Belgium, and is part of the investigator driven study to explore potential indications of an intraoperative specimen PET-CT imager (Trial registration number: BUN: B0172022000009).
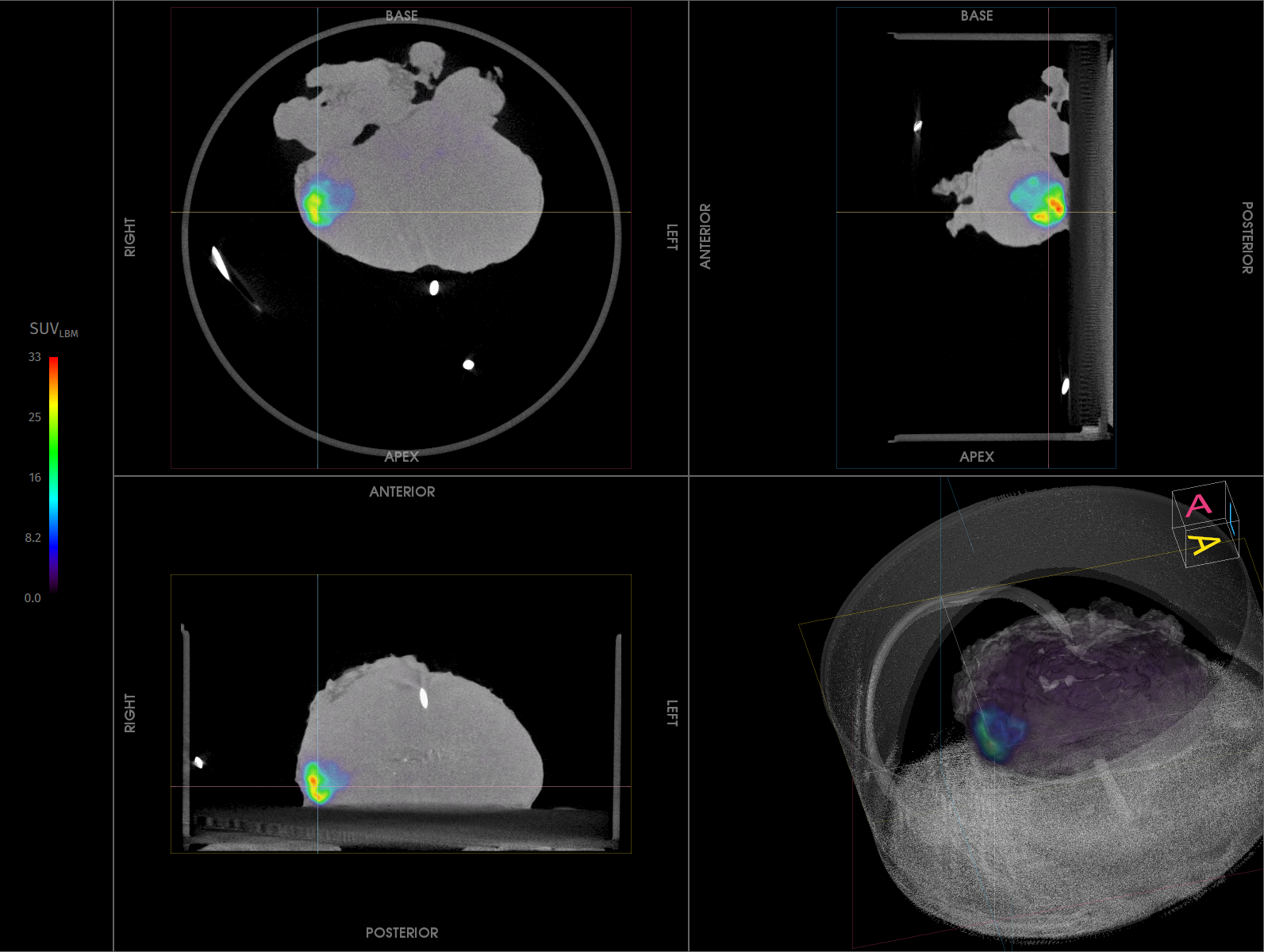
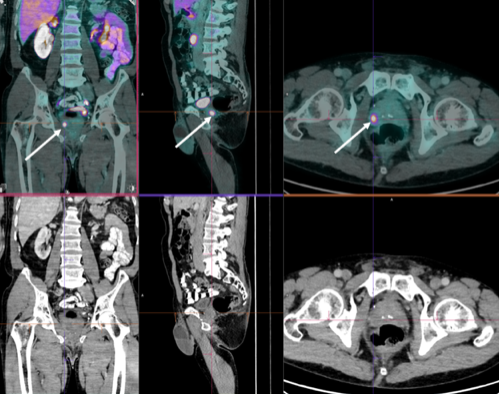 Figure 1. Pre-operative 18F -PSMA PET-CT image, acquired twelve weeks before surgery. High uptake is shown at the right posterior zone of the prostate, with SUVmax of 15.64.
Figure 1. Pre-operative 18F -PSMA PET-CT image, acquired twelve weeks before surgery. High uptake is shown at the right posterior zone of the prostate, with SUVmax of 15.64.
Patient History
Specimen PET-CT images
The patient was intravenously injected with 1 MBq/kg of 18F-PSMA at the start of the surgery.
Resection of the prostate specimen was completed 88 min post-injection. Immediately after resection, a high-resolution specimen PET-CT image was acquired in the operating theatre. The images are shown in Fig. 1. In this image three orthogonal views of the specimen PET-CT images are seen. The PET images are represented in color scale, superimposed on the CT images in greyscale. The images of the prostate specimen clearly show increased 18F-PSMA uptake with SUVmax of 33. At the right posterior zone of the specimen, 18F-PSMA uptake is seen close to the border of the specimen.
Figure 2. Transverse, coronal, and sagittal slices and 3D view of the specimen PET-CT images of the prostate specimen. Specimen orientation is as indicated. The tumor is represented by a bright colorful region in the specimen. The PET tracer scale bar is depicted on the right-hand side. At the right posterior zone of the specimen, 18F-PSMA uptake is seen close to the border of the specimen.
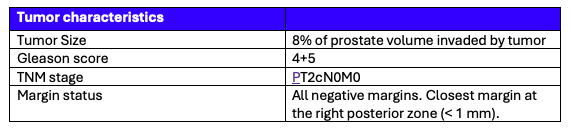 Table 1. Tumor characteristics assessed by histopathological evaluation.
Table 1. Tumor characteristics assessed by histopathological evaluation.
Histopathological evaluation
After specimen PET-CT imaging, the surgical specimen was sent to the pathology department for routine histopathological evaluation, which was available after several days. The histopathological results are listed in Table 1.
All surgical margins were found negative, with closest margin at the right posterior zone of the specimen. This correlates with the regions of high radiotracer uptake on the specimen PET-CT image.
Discussion and conclusion
Radical prostatectomy requires a delicate balance—removing cancer while preserving nerve structures critical to quality of life. A nerve-sparing approach reduces the risk of postoperative impotence and incontinence, but it also increases the challenge of ensuring complete tumor removal. Therefore, having real-time insights on whether the tumor has been fully resected is highly valuable during nerve-sparing surgery.
In this case, the specimen PET-CT images show an excellent correlation with histopathology. The images specifically highlight radiotracer uptake close to – but not reaching - the border of the right posterior zone of the specimen where histopathological analysis finds indeed a close surgical margin.
Therefore, this case shows how intraoperative specimen PET-CT imaging with 18F-PSMA can visualize the tumor in the resected tissue specimen and can help surgeons make informed, real-time decisions, ensuring optimal cancer removal while preserving critical structures. The result? Greater confidence, which may lead to enhanced precision, and improved patient outcomes.
References
[1] Darr C et al. (2023). Intraoperative Molecular Positron Emission Tomography Imaging for Intraoperative Assessment of Radical Prostatectomy Specimens. European Urology Open Science 54:28-32
[2] Okarvi, S. M. et al. (2019). Recent developments of prostate-specific membrane antigen (PSMA)-specific radiopharmaceuticals for precise imaging and therapy of prostate cancer: an overview. Clin. Transl. Imaging 7:189–208. issn: 22817565
[3] Muraglia L et al. (2023). First Live-Experience Session with PET/CT Specimen Imager: A Pilot Analysis in Prostate Cancer and Neuroendocrine Tumor. Biomedicines 11:645.
[4] Lambert B. et al. (2025) Feasibility study on the implementation of a mobile high-resolution PET/CT scanner for surgical specimens: exploring clinical applications and practical considerations. Eur J Nucl Med Mol Imaging. https://doi.org/10.1007/s00259-025-07143-z
[5] Moraitis A. et al. (2025) Evaluation of Surgical Margins with Intraoperative PSMA PET/CT and Their Prognostic Value in Radical Prostatectomy. jnumed. 124.268719. https://doi.org/10.2967/jnumed.124.268719